- Various studies have demonstrated that treatment with methyl prednisolone and chlorambucil could increase the chance of remission of idiopathic nephrotic syndrome (INS) of varied histology in patients who do not respond to the conventional treatment. This study was done to assess the safety and efficacy of methyl prednisolone and chlorambucil regimen in patients with various types of glomerulonephritides which were resistant to the usual conventional immunosuppressive drugs. Thirty nine patients were treated between June 1998 and December 2003 with Ponticelli regimen for six months. Twenty three patients (58.98%) were men and 16 (41.02%) were women. Mean age at the onset of NS was 23.59 ± 1.28 (range 10-51) years. Four patients (10.2%) had minimal change disease (MCD), six patients (15.4%) had membranoproliferative glomerulonephritis (MPGN), two (5.1%) had IgA nephropathy, and 18 patients (46.1%) had focal segmental glomerulosclerosis (FSGS). Eleven patients were excluded from the final analysis. Of the remaining 28 patients, mean baseline proteinuria was 3.31 ± 3.09 g/day. Mean baseline plasma albumin was 2.84 ± 1.002 g/dl and mean baseline serum creatinine was 0.87 ± 0.42 mg/dl. At the end of six months of treatment, mean proteinuria was 1.02 ± 0.85 g/day. Mean plasma albumin was 3.69 ± 0.78 g/day, and mean serum creatinine was 0.85 ± 0.26 mg/dl. Mean followup was 13.21 ± 7.7 times in 18.92 ± 12.58 months. At the end of six months of treatment, seven patients (25%) achieved complete remission (CR), 10 patients (35.71%) partial remission (PR), and 11 patients (39.3%) did not show any response to the therapy. Most of the patients in responder group had FSGS (64.70%), whereas in nonresponder group patients had MPGN and mesangioproliferative glomerulonephritis (MesPGN). Out of 13 FSGS cases five (38.46%) achieved CR, six (46.15%) PR, and only two (15.38%) failed to respond. The incidence of side effects was 39.3%. Responders had more side effects than nonresponders (47 vs 27.3%). Methyl prednisolone and chlorambucil therapy (Ponticelli regimen) is safe and efficacious in achieving remission in significant number of INS patients other than membranous nephropathy, without any serious side effect on short term followup. However, a longer followup is required to demonstrate the sustained efficacy and long-term side effect of this regimen.
-
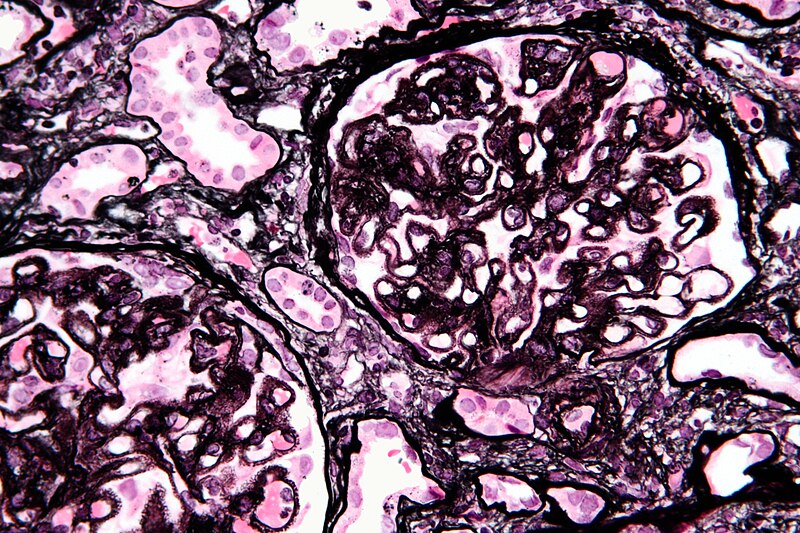
Membranous nephropathy
Primary/idiopathic
- 85% of MGN cases are classified as primary membranous glomerulonephritis -- that is to say, the cause of the disease is idiopathic (of unknown origin or cause). This can also be referred to as idiopathic membranous nephropathy. One study has identified antibodies to an M-type phospholipase A2 receptor in 70% (26 of 37) cases evaluated.[4]
Secondary
- autoimmu
- The remainder is secondary due to:
- infections (e.g., syphilis, malaria, hepatitis B)
- drugs (e.g., captopril, NSAIDs, gold, mercury, penicillamine, probenecid).
- inorganic salts
- tumors, frequently solid tumors of the lung and colon; hematological malignancies such as chronic lymphocytic leukemia are less common
Treatment
- Treatment of secondary membranous nephropathy is guided by the treatment of the original disease. For treatment of idiopathic membranous nephropathy, the treatment options include immunosuppressive drugs and non-specific anti-proteinuric measures.
Immunosuppressive therapy
- Corticosteroids: They have been tried with mixed results, with one study showing prevention of progression to renal failure without improvement in proteinuria.
- Chlorambucil
- Cyclosporine
- Tacrolimus
- Cyclophosphamide
- Mycophenolate mofeti
Natural history
- About a third of patients have spontaneous remission, another third progress to require dialysis and the last third continue to have proteinuria, without progression of renal failure.
Monday, 20 February 2012
Ponticelli regimen in idiopathic nephrotic syndrome

Subscribe to:
Post Comments (Atom)
No comments:
Post a Comment